Superior Index Go to the next: Chapter 10
Print Files: A4 Size.
Five years ago, Chuck Holmes was at the top of his game. His uncanny ability to crank out one astonishing achievement after another in the high tech world of computer programming and digital design had catapulted him into the highest realms of geekdom. In 30 years he had progressed from 80's whiz kid to primo west coast web designer.
Youthful, exuberant, creative, and generous, Chuck smiled and joked his way into people's hearts. Everybody liked him. You know the type: bright but not obnoxiously so, ready to help, usually the center of attention, and always able to summon an incisive comment that cuts to the core of the matter.
Chuck worked hard and played hard. He was in love with his wife and his two boisterous teenage boys. His diet was ideal: plenty of fruit and vegetables, whole grains and beans. All organic. Low carb, no sugar, no white flour. Almost no animal fat. Trim and fit, Chuck played tennis on the days he didn't work out at the gym.
Chuck paid close attention to his health and it seemed perfect. He saw his doctor for regular checkups and his lab tests always came back normal.
Healthwise, he did everything right. ... or so it seemed.
Then, suddenly, one sunny Monday morning on the way to his office, Chuck felt a sharp pain in his chest. He collapsed and was taken to the ER, where he was told he was having a heart attack. An angiogram the next day revealed major atherosclerotic disease affecting all four coronary vessels. The next day a quadruple bypass was performed on him. Chuck had had a busy week.
"In an office visit between his heart attack and his bypass surgery, Chuck rather pointedly asked his internist, `My cholesterol and LDL have always been normal. My HDL is high. On several occasions you've told me that I had the `heart of a racehorse,' and that my coronary risk factors were `very low.' Now this! What went wrong?' "
"Dr. Turner replied, `I am so sorry, Chuck, but I honestly don't know. Some people who have normal cholesterol levels still can have heart attacks.' (By now I hope you realize what an understatement that was.)"
Chuck wasn't getting helpful answers from his regular doctors, so he decided to enlist my help. I tested him, and discovered that his homocysteine had gone through the roof.
So what was it that caused Chuck's coronaries to harden? It wasn't cholesterol; his was low. It wasn't a sedentary lifestyle; he was active. It wasn't obesity, his weight was perfect. It wasn't diet; he ate right. The answer is that Chuck had a very common (but rarely diagnosed) disorder known as hyperhomocyteinemia - a five dollar word for too much homocysteine in the bloodstream.
What the heck is homocysteine, why is it dangerous, and why did Chuck have too much of it?
Homocysteine is a small, sulphur-containing amino acid molecule that our bodies generate in the process of recycling the essential amino acid methionine. Why be concerned about an obscure molecule that's part of an equally obscure biochemical process? Because a little too much homocysteine in your bloodstream can cause many diseases, and it can even kill you. In this section I will describe how homocysteine damages the heart and vascular system. In the following section, I will enumerate the many other diseases that are either caused or exacerbated by excess homocysteine.
As you know from Chapter 5, the endothelium - that delicate, one cell thick inner protective lining of our blood vessels - is continuously exposed to thousands of potentially damaging chemicals floating in the bloodstream. These irritants cause heart disease. Homocysteine, because it attacks and destroys important vascular protein molecules, is one of the nastiest.
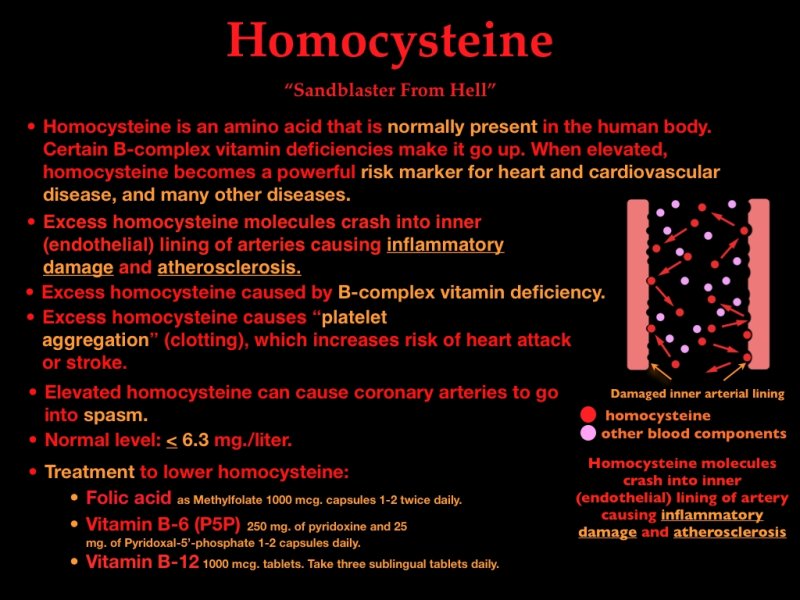
Low levels of homocysteine are normally present in the human body. However, as long as levels stay below 6.3 μmol/L, they won't cause any damage. When homocysteine rises above this safe cutoff point, the endothelium begins sustaining major damage. Like a powerful mini sand blaster, billions of homocysteine molecules crash into endothelial cells, irritating and damaging them. A chronically irritated endothelial lining loses its integrity and can no longer protect the layers of artery beneath it. The borders between the endothelial cells weaken, and begin allowing cholesterol-laden oxidized LDL particles and other pro-inflammatory chemicals to squeeze past and gain access to the arterial wall (the intima) beneath. Over time this molecular pounding results in arterial inflammation, plaque, atherosclerosis, and thromboembolic disease.
"Is homocysteine useful for predicting anything other than heart disease risk?" asks Chuck.
"Yes, it is. The homocysteine story doesn't just end with heart and cardiovascular disease. Homocysteine doesn't limit its vandalism to injuring arteries; it can cause inflammation anywhere and everywhere in the body, and this means that those with a high homocysteine are at higher risk for a striking array of diseases, including (but not limited to) macular degeneration, Crohn's disease, ulcerative colitis, inflammatory bowel disease, aortic aneurysm, depression, bipolar disorder, schizophrenia, cervical cancer, Parkinson's disease, and even birth defects."
"Well, Chuck, there's no reason to think a fetus can't be adversely affected by too much homocysteine."
"Also, a buildup of homocysteine has an especially deleterious effect on sensitive brain tissue and cerebral function. High homocysteine levels damage the brain by fracturing important neuronal proteins and by ravaging the brain's arterial supply lines. There is a close association between high serum homocysteine levels and neuropsychiatric disorders. Many studies have found a connection between hyperhomocysteinemia and impaired cognitive performance."
"You mean it could cause senile dementia?" asks Chuck.
"Yes, alterations in cognitive function are seen in people with elevated homocysteine, ranging from mild cognitive decline - age-associated memory loss - to vascular dementia, and other senile brain syndromes including Alzheimer's and Parkinson's. A homocysteine level above 14 amplifies your risk of Alzheimer's and other neurodegenerative disorders by a whopping 150%. Physicians often misdiagnose these changes as "normal aging," but they are a preventable, reversible phenomenon."
"Anything else homocysteine can do?" asks Chuck pensively.
"Numerous researchers have identified an association between cancer and impaired homocysteine metabolism. By disrupting collagen formation in bone, high homocysteine levels double the risk of osteoporosis. Population studies have shown that the higher a person's homocysteine level the shorter their life expectancy. I could go on and on, but you get the idea. It affects everything."
The damage caused by homocysteine extends far beyond the cardiovascular system. As mentioned above, homocysteine excess is causally associated with body-wide risk for a plethora of chronic diseases, including osteoporosis, memory loss, cognitive impairment, senile dementia, Alzheimer's disease, diabetes, fibromyalgia, chronic fatigue syndrome, birth defects, depression, rheumatoid arthritis, multiple sclerosis, and cancer. Though this is a disparate group of disorders, the fundamental pathogenic mechanism is the same: a toxic molecule (homocysteine) irritates and damages sensitive protein molecules. This triggers a chronic inflammatory reaction that causes ongoing cellular damage. When nerve cells are targeted, the result is Alzheimer's, senile dementia, multiple sclerosis, memory loss, depression, etc. When bone cells are damaged, we see increased fractures in the elderly. When joints are attacked, you get arthritis, and when a developing fetus is the target, we see birth defects. When cells of the cardiovascular system are ravaged by too much homocysteine, we see heart attacks, strokes, and other vascular diseases. The following brief summary of research results from thousands of studies depicts the tip of a huge iceberg:
Osteoporotic fractures in the elderly are far more frequent in those with high homocysteine. Women with high homocysteine levels have significantly lower hip bone mineral density than controls.
Cognitive function is affected by high homocysteine levels. Numerous studies have linked elevated homocysteine levels to vascular dementia and Alzheimer's disease. Dementia has also been associated with reduced levels of folate and vitamin B12.
High homocysteine levels are associated with increased risk of several complications of pregnancy. Abnormal homocysteine affects the developing fetal nervous system causing neural tube birth defects. In one large study, scientists found that pregnant women with the highest homocysteine levels had an increased risk of premature births, low-birth-weight infants, and stillbirths. Folic acid supplements have been shown to help prevent these birth defects.
Women with higher homocysteine have a significantly higher risk of colorectal cancer and cervical cancer than women with lower levels.
High levels of homocysteine predispose individuals to inflammatory bowel disease: ulcerative colitis and Crohn's disease.
More than half of patients with severe depression had elevated homocysteine levels and decreased levels of folate.
Young men with bipolar (manic depressive) disorder have higher homocysteine levels.
Many schizophrenia patients have high homocysteine levels. When vitamins were used to reduce the homocysteine, their symptoms of schizophrenia lessened.
Patients with age-related macular degeneration have higher homocysteine levels than healthy subjects.
From the above it becomes clear that anyone interested in optimum health and longevity would do well to check their homocysteine level and correct it with natural medicine if elevated.
Methyl (CH3) groups - simply a carbon atom surrounded by three hydrogen atoms - are basic building blocks our bodies use in protein synthesis. We need a continuous supply of methyl groups to generate the tens of thousands of proteins our DNA is programmed to deliver.
Methionine, an amino acid in foods we eat, carries and delivers methyl groups. We call this "methylation", and methionine acts as a "methyl donor".
If we are nothing else, we humans are huge protein-synthesizing factories. (I don't want you to think that this is all we can do, but it is a good start.) Our genes are programmed to make the enzymes (which also are proteins) that catalyze the synthesis of vast numbers of proteins used for every conceivable bodily function, including organ and tissue maintenance, hormone synthesis, immunity, stress control, inflammation management, and healing. Proteins are likewise in great demand for repairing, removing, and replacing old or damaged cells. Methylation is a crucial part of this process. To supply enough methyl groups for all the proteins that are being synthesized to maintain and repair our bodies, we need to be able to methylate - and recycle methionine - like crazy.
The methionine recycling pathway, one of thousands of biochemical pathways, provides an especially important biochemical function because it stores and delivers one of our bodies' most basic chemical building blocks: methyl groups. Here's how the methionine recycling pathway works. When methionine "delivers" a methyl group, it becomes S-adenosyl-methionine (SAMe), which now needs to be recycled back into methionine. On the way back to becoming methionine, SAMe can be converted into one of two amino acids: homocysteine (which we know is damaging) or cysteine (which is harmless). If conditions are right (and this is a big "if" as you will soon see), homocysteine is instantly converted back into methionine, which, now replenished, can go back out and deliver more methyl groups. Inadequate supplies of three B- complex vitamins - folic acid (as L-methylfolate), B-6 (as pyridoxine-5-phosphate), and B-12 - will stall the recycling process, causing unwanted homocysteine to build up in the bloodstream. A long-term deficiency of B-6, folic acid, or B-12 causes a homocysteine buildup. It's like that famous "I Love Lucy" episode where Lucy and Ethel get a job in the chocolate factory and they can't keep up with the production line. Homocysteine, like the chocolates on Lucy and Ethel's conveyor belt, backs up, overflows, and spills out into our bloodstream - and that spells trouble. Like billions of tiny angry sharks, excess homocysteine molecules ravage the inner endothelial lining of our arteries, causing damage, inflammation, dysfunction, cell proliferation, plaque, clot formation, atherosclerosis - and, ultimately thromboembolic disease.
Mainstream and alternative doctors agree that simply replacing the trio of B-complex vitamins (using optimum doses, of course) usually solves the problem. Less often (about 15-20% of the time), a shortfall of choline, S-Adenosylmethionine, trimethylglycine, and/or zinc is responsible for the obstruction in methionine recycling. I'll discuss these in the section on treatment.
No one questions that B vitamins lower homocysteine levels, but does this lowering translate into disease prevention or reversal? This idea has never been appropriately tested. Two major studies (Bonaa, NEJM 2006 and Albert et al., JAMA 2008), however, have succeeded in misleading physicians into thinking that homocysteine reduction is useless. In the first study, the Norwegian Vitamin Trial (NORVIT) published in the New England Journal of Medicine in 2006, Bonaa et al. reported on almost 4000 individuals with late-stage heart disease who had been recruited within a week of having experienced a myocardial infarction. These patients suffered from advanced cardiovascular disease - the kind that has been brewing for decades. Most of the subjects had normal homocysteine levels. After giving these patients small doses of B vitamins for two months, the authors concluded that this treatment was ineffective for reversing heart disease. A random person on the street could tell you it's unlikely that B vitamins could cure heart disease at all, much less in two months. Does it strike you as odd that none of the 100 doctors participating in this study realized how ludicrous this idea was?
A second study, published a couple years later (Albert, JAMA 2008) tried giving B vitamins to women at high risk of cardiovascular disease, again with the deluded expectation that vitamins could cure them. Multiple risk factors had been traumatizing these patients' arteries for decades, causing oxidative stress, inflammation, endothelial cell damage, endothelial dysfunction, plaque formation, thrombosis, and cell proliferation - finally causing so much cumulative damage that a blockage in a major coronary vessel had occurred. B-complex vitamins - properly prescribed - might have helped prevent these infarctions, but it's a bit of a stretch to expect reversal of extensive damage. Providing B vitamins to heart attack victims would be about as likely to help as handing out tinker toys to after a tornado and expecting rebuilt homes.
Though there were multiple flaws in this study (see below). The most egregious, I believe, was the failure to examine and document all the heart markers discussed in this book. Heart attacks are multi-causal events, but Albert's study was based on the scientifically unsupportable - and truly unreasonable - assumption that all heart attacks are caused by B vitamin deficiencies and/or too much homocysteine. Failure to identify and address all the factors that caused their patients' disease doomed this study from the git-go.
There is no shortage of misguided research studies out there, and here we have two blatant examples. These studies proved what any reasonable person would expect: administering B vitamins to people who have just had a heart attack will produce no cures. Lowering homocysteine clearly helps prevent heart attacks and strokes (and senile dementia, osteoporosis, fibromyalgia, arthritis, cancer, etc.), but no expert in nutritional biochemistry would suggest that vitamins could cure them. Unfortunately, these high-profile studies deluded many doctors. Homocysteine-lowering as a way to prevent major cardiovascular casualties was stoned back to the Dark Ages. Here are the fundamental reasons why these studies should be tossed into the medical research trash can:
Studies have already shown - beyond any shadow of doubt - that homocysteine tears apart crucial cellular protein molecules, causing the horribly disfiguring nanoscale cellular damage that initiates atherosclerosis and numerous other disease processes. Hundreds of basic science research papers have already show that less homocysteine translates into less damage.
Meanwhile, the misconceptions persist and homocysteine remains the misunderstood Charlie Brown of biochemicals. Just about any conventional doctor will tell you these studies showed "B complex vitamins don't cure patients with heart disease."
Information about homocysteine is widely available. Most doctors are at least aware of it. No expert questions that an elevated homocysteine can predict a future heart attack better than an elevated cholesterol. Had his doctor ordered this inexpensive test, Chuck's homocysteine problem could have been diagnosed before any symptoms appeared, and a few cheap B-complex vitamins could have reversed his disease. Instead, homocysteine molecules beat up on Chuck's coronary arteries for 20 years, corroding them and gradually setting the stage for a cardiovascular nightmare. All physicians should include an annual homocysteine level in their routine screening panel.
Chuck's doc is not alone, however. Most physicians neglect to order a homocysteine level, an error of omission that in effect bestows a death sentence on millions of people - men and women alike - who, like Chuck on the way to bypass surgery, might be wondering why their doctor told them, "No worries; your cholesterol is fine."
"Chuck's initial office visit was just a few days after his bypass. Before his visit, I had ordered my usual cardiovascular risk panel. All of Chuck's risk factors but one were entirely in the normal range. The exception was his homocysteine, which was elevated at 18 μmol/L."
"In going over his results, I explained to Chuck: `Homocysteine is an `independent risk factor' for coronary artery disease. Homocysteine is an amino acid molecule that is normally present in the body, and low levels of it are not going to hurt you. When levels rise, however, this molecule goes morphs into a killer.' "
"What is a healthy homocysteine level, doc?"
"Homocysteine is measured from a blood sample taken after a twelve hour fast. A normal homocysteine level is at or below 7 micromoles per liter (μmol/L). I like to see it below 6.3; above that number we start seeing risk. Based on a ton of research, that's optimum. Between 7 and 10 there is significantly increased risk, and risk gets very high above 10."
"Thirteen. That's high by anyone's standards."
"How does homocysteine damage my blood vessels?"
"Chuck," I explained, "the inner lining of your arteries - we call it the endothelium - is one cell layer thick. It acts as a highly selective membrane with two jobs. The first is to sort through all the chemicals floating in your bloodstream and allow passage of those that are desirable while keeping the unwanted ones out. The second job is to protect the arterial cells beneath it from irritants and toxic chemicals. This endothelial lining of your coronary arteries is very delicate and sensitive, and homocysteine molecules have been banging up against it for years now, causing inflammation and cumulative damage - in other words, plaque.
"Homocysteine," I continued, "also makes your blood more likely to clot, (technically we call this platelet aggregation) and this is not good because that clot - or thrombus - may block an artery and cause a heart attack."
"Yes. Also, as a separate effect, homocysteine can cause coronary arteries to go into spasm, which is not what you'd want if the vessel were blocked by a clot."
"Yes, and it is appalling that your homocysteine hadn't been measured until now! It's far better at predicting cardiovascular disease than cholesterol, and there is no doubt that homocysteine played a significant role in your heart attack."
"If it's so important, why didn't my cardiologist - or my primary care doctor for that matter - why didn't they check my homocysteine out?"
"Good question. Wish I had a good answer."
"How do I get mine back down to normal?"
"Lowering homocysteine is easy, inexpensive and virtually always effective. That's why its such a shame yours wasn't checked earlier. Prevention is always easier than cure. This one little test could have saved you much grief. To lower your very high homocysteine of 15 down to the 5.0-7.0 that I'd like to see, I want you to take the following three B-vitamins: folic acid (as L- methylfolate 1000 mcg tablet, 1-2 twice daily), vitamin B-12 (as 1000 mcg 1-2 sublingual tablets twice a day), and vitamin B-6 (as pyridoxine-5-phosphate 50 mg capsules) 50-200 mg twice a day."
"These vitamins are coenzymes that facilitate the pathways that metabolize your excess homocysteine, breaking it down into methionine. A deficiency of the vitamins causes less homocysteine to be transformed back into methionine, so the homocysteine builds up in the bloodstream. Taking B-6, B-12 and folic acid revitalizes the transformation of homocysteine into methionine so your homocysteine level will gradually go down, and less homocysteine means less inflammatory irritation to the endothelial membrane and other sensitive structures throughout the body.
"Although," I continued, "most people respond to the standard triple vitamin regimen I just described, a small percentage is metabolically different and may need other nutrients (see Plans A and B below) to bring down their homocysteine. This is because there are several possible metabolic disruptions that can cause homocysteine to build up, so if after three months the standard treatment (folic acid, B6, B12) hasn't worked for you, don't give up. Simply try the other possibilities (listed below). Keep testing every three months and changing your program until you find the combination that works best for you. Don't settle for a slightly lower homocysteine! You want to get it down to 7.0 or less, and you want to keep it there permanently. This is the only way to assure zero risk of the many diseases caused by an elevated homocysteine."
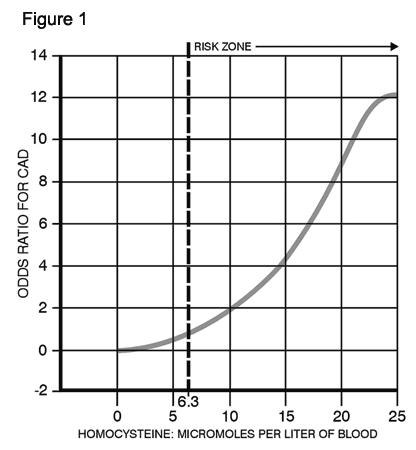
As seen in the graph below, risk gradually rises in tandem with homocysteine level. Experts choose to use a cutoff point of 6.3, below which there is no demonstrable increased risk of heart attack or stroke. Above 6.3, risk gradually rises. At 10, risk is about double baseline; at about 12 it is triple; at 15 quadruple.
Don't be surprised if the "normal" values for homocysteine that appear on laboratory reports and research studies are higher than the numbers I give here. This may be because the curve accelerates above 15 (i.e., is steeper) up to 25 - but we are not statistics, we are individuals who desire optimum health, so even minimal risk is unacceptable.
The rest of Chuck's story is an inspiring medical success. He addressed the challenge of lowering his homocysteine with typical enthusiasm. He followed the treatment program (provided at the end of this chapter) and over the following nine months his homocysteine gradually returned to normal. Freed from the constant inflammatory damage, Chuck's coronary arteries slowly healed and he gradually got back to his life of work and travel. He returned to his busy computer consulting business, resumed his regular tennis, and booked a summer cruise to Norway with his wife and kids. It hadn't been too late to reverse the damage to his blood vessels.
Finding and treating his elevated homocysteine happened just in time for Chuck. Without treatment, his prognosis was less than rosy.
For the most part, Chuck's medical care had been superb: great docs, state-of-the-art CAT scans, EKGs, echocardiograms, angiograms, clot-busting drugs, and deft surgical techniques. Prevention, the most powerful medicine of all, had not been part of the picture. Beyond cholesterol measurement and a low animal fat diet, there had, in fact, been no prevention. This was unfortunate, though typical: mainstream medicine, for all its sophisticated technology, assigns lower importance to prevention than to treatment. Perhaps this is because there's less money in it, or because herbs and vitamins are poorly understood by conventional doctors. Whatever the reasons, our current system depends on a constant supply of new heart attacks, without which all that high tech equipment would just collect dust. The mortgage payment would still be due, but there'd be no revenue to cover it. Are you with me here? The monster is not happy when it is hungry.
Then there's the thrill of the heart attack (as long as it's not your own), the kind of medical excitement that drives millions to watch Gray's Anatomy reruns. With prevention, the thrill is gone; it's borring. How do you know you prevented anything (like, say, a myocardial infarction or a stroke) if it never happens? (Answer: for a specific person, you can't; for populations, you can.)
Chuck was lucky; he sidestepped the fate of millions. Senseless death is not the exception; it's the rule. Testing and treating, as outlined in this book, could prevent almost all heart attack deaths.
Though multiple positive risk factors generate even higher risk, an elevated homocysteine alone - that is, without an elevated cholesterol or LDL, and without elevations of any of the other risk factors for heart disease - can cause a heart attack or a stroke. Chuck was a perfect example. Conversely, lowering your homocysteine to 6.3 μmol/L or less removes homocysteine as a risk factor, but will not negate the risk of a high cholesterol or an elevated CRP. Every "independent risk factor" must be addressed and treated. The more risk factors you identify and remove, the lower your overall risk of heart attack and stroke. Eliminating them all places risk at very close to zero.
Lower homocysteine to ideal level of 6.3 μmol/L or less.
L-Methylfolate - an efficiently absorbed form of folic acid Dose: 800-1000 mcg. tablets. Take 2-4 daily.
Vitamin B-6 (pyridoxine). Take as the active form, P-5-P (pyridoxine-5-phosphate). Best products combine pyridoxine with P-5-P in a 9:1 ratio; 275 mg. per capsule. Take 1-3 capsules daily.
Vitamin B12 as methylcobalamin (important because other forms of B12 are not absorbed), 1000-5000 mcg daily (can be taken in one daily dose).
Combined B12 methylcobalamin/methylfolate products have recently become availble (e.g., Renewal Research "Active B-12 - Folate"). These make dosing easier by combining in one tablet the most active, most absorbable forms of both folic acid (5-methylfolate) and B12 (methylcobalamine). Take 2-4 tablets daily, dissolved in the mouth or swallowed whole.
It is important to take all three of the above B-complex vitamins, as the effects are synergistic.
As mentioned above, there are several possible biochemical causes of an elevated homocysteine. There is no test to determine which of these causes applies, so a little trial and error is required. The most common cause of elevated homocysteine (about 70%) is a deficiency of B-complex vitamins: folic acid, vitamin B-6, and/or vitamin B-12. Therefore, replacing these three vitamins is always the starting point. This is Plan A below. Most people will respond to the folic acid, B-6, and B-12 regimen.
To make sure your homocysteine-lowering program is on track, you will want to retest your homocysteine level every two months or so. Remember, homocysteine levels change slowly (we are talking months here), so you are looking more for a direction of change than for a normal result. In other words, if, compared to your previous result, your level is going down, even just a little, you know you are on the right track and that you should continue on your current program. If your retest level is not lower, then you are still not addressing all the possible biochemical causes of the nutritional deficiency that is causing your homocysteine to rise. About 15-25% of people will not respond to Plan A alone, so if you are not showing any response after two or three months, add the nutrients in Plan B. Testing every 2-3 months (until you establish that you are consistentlymoving in the right direction) will be necessary to determine which combination of nutrients you need.
If you are among the 15-25% of people who won't respond to the above Plan A regimen, your homocysteine elevation was not caused (at least not solely caused) by a shortfall of folic acid, B6, and/or B12. The focus now shifts to a possible deficiency of other nutrients that facilitate removal of excess homocysteine. These include choline, S-Adenosyl methionine (SAMe), and trimethylglycine (TMG-also known as betaine, a B-complex vitamin). If a two month trial on these supplements lowers the homocysteine (even just little) you'll know a deficiency of one or more of these nutrients is part of your homocysteine problem. (Do not discontinue the P-5-P, methylfolate, and B12 during this trial as these may still be part of the problem.)
It is best to try all three of these nutrients together, because they reinforce each other's action. If, on retesting, you see a homocysteine reduction after 2-3 months, try going off one or two of the three to figure out which is working. If no homocysteine reduction in three months, discontinue all three, as they are not working.
It is important to appreciate that getting homocysteine to normal/baseline (i.e., ≤ 6.3) is not the immediate goal here. That could take up to a year or more, as homocysteine levels move down very slowly. Any movement in the desired downward direction would indicate the nutrient combination you are taking is working and that you should stay the course.