Superior Index Go to the next: Chapter 5
Print Files: A4 Size.
Like ostriches with our heads in the sand, we are living in the midst of a modern epidemic, oblivious to the fact that most of us will succumb to it.
Coronary artery disease is - by far - the biggest killer of all. Stroke is number three. No other modern illness comes close to reaping as grim a toll on human life as atherosclerotic cardiovascular disease. The term "epidemic" fails to capture the enormity of this public health problem. Consider these staggering statistics:
Whether measured in terms of human suffering or dollars, the cost of this epidemic is outrageous - and unnecessary.
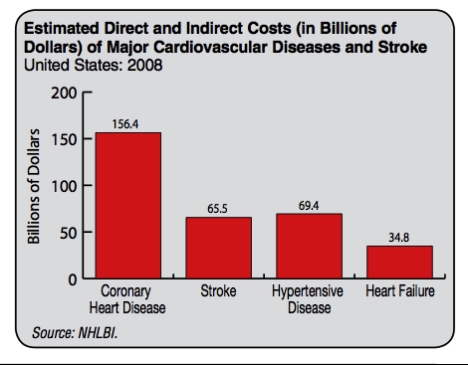
"Gargantuan" would be a reasonable term to describe the economic impact of cardiovascular disease on the U.S. health care system. The Centers for Disease Control (CDC) estimates that the cost of heart disease and stroke in the United States exceeded $500 billion in 2010. By way of comparison, the total annual budget, at around 2 trillion, is only four times as much. To quote the late Senator Everett Dirkson of Illinois, "A billion here, a billion there, and pretty soon we're talking real money."
Coronary artery disease has spawned a multibillion dollar industry that features advanced techniques that generate huge profits for the "medical-industrial complex". Bypass surgery, balloon angioplasty, cardiac catheterization, stents (a wire meshed affair that is inserted inside a blocked artery to keep it open), and prescriptions for an array of expensive, symptom-suppressive, high-tech drugs. It isn't as if these methodologies don't work; they do - at least in the short run. But none of the sophisticated tools described above addresses the actual causes of vascular disease, so it progresses regardless. Bypass surgery and its ilk are useful only after the disease has become life threatening. Why not enable prevention by putting more of those big bucks into addressing the causes of the disease?
The irresistible profitability of modern cardiovascular medicine creates a huge problem. Prevention - though relatively inexpensive and easily attainable - isn't capable of generating the kinds of insane revenue streams as drugs and surgery. Prevention, in fact, erodes profits by removing future customers. It starves the beast and therefore threatens the very existence of the extremely lucrative coronary artery disease industry.
This human tragedy can now be averted by detecting the earliest stages in the development of heart disease. This can be accomplished long before symptoms appear. When abnormal test results reveal dark clouds on a patient's cardiovascular horizon, we now possess the technology to reverse the risk. Modern cell biology has delivered a detailed understanding of the evolution of the atherosclerotic disease process (see Atherogenesis, Chapter 5). We can "see" the biochemical fingerprints of atherosclerosis long before overt symptoms appear. Using the heart markers described in this book, we can sort through the complexities of cell biological function, identify the disruptive forces, and then fix them before they cause a disaster. At this point in the evolution of our understanding of cardiovascular disease, only a handful of physicians apply the revolutionary molecular medical discoveries of the past ten years that allow us to identify and prevent or reverse atherosclerosis. Most doctors continue to adhere to the tragically archaic notion that all they need to do is lower cholesterol and blood pressure (with the appropriate drugs, of course - a statin here, a calcium channel blocker there), suggest a low-fat diet and some exercise, and voila! - "prevention".
The cardiovascular industrial medical complex and its 25-billion-dollar statin industry wants to keep the doctors - and you - thinking that all you'll ever need are drugs and surgery. We need to question the "experts" who insist on waiting until heart disease has reached an advanced state, and then roll out the very profitable hardware of medical desperation. Millions of lives would be saved by altering our approach. Researchers have identified and extensively characterized the molecular "risk markers" that are causally related to heart attack and stroke. Though it may take the health care delivery system decades to shift over to early identification, you can implement these discoveries on a personal basis right now. Get the tests listed below. If any of your markers are abnormal, you know you are at risk, and by studying the chapter that discusses that marker you will know exactly why you are at risk. I'll explain what you need to do to repair the malfunctioning biochemical system so that the marker - and your heart disease risk - returns to normal. Retesting will tell you whether your program is working.
Doctors need to understand that the key to preventing heart attacks and strokes is early detection (in other words, testing for the six heart markers described below). Abnormal markers need to be treated with gentle natural medicines. Reversing the abnormal markers will halt the progression of the disease process, and go on to reverse it. Detecting atherosclerosis in its early, reversible stages allows the use of gentler, plant-based medicines that support the body's healing systems. This obviates the necessity of using toxic drug medications that mask the symptoms.
The six heart markers I recommend for identifying the underlying causes of heart attacks and strokes are:
An elevation of any one of these markers spells trouble. Taken together, these tests constitute an exceptionally accurate set of tools for predicting cardiovascular risk, for identifying this disease before it happens - and for reversing it before it maims or kills.
Everyone is different. You might have elevated cholesterol and fibrinogen, while your friend might have elevated homocysteine, C-reactive protein, and fasting blood glucose. Any combination of markers is possible, so, when it comes to treatment programs, there can be no "one size fits all".
The chapters in Part II of this book are devoted to these markers. Each is described in greater detail with a focus on the role each plays as a causative agent in atherosclerotic heart and cardiovascular disease. I'll show you how to design your own personalized prevention and/or reversal program using natural, food-derived, nontoxic nutritional medicines that will lower each marker gently back to normal. Retesting at regular intervals will help you track your progress and determine whether your treatment program is working.
I list the cholesterol (lipid panel) first only because it is the most familiar. If I were listing the markers in terms of their predictive capabilities, the lipid panel would come in dead last.
Identifying and correcting each of these additional markers will further increase your protection from the "Number One Killer":
This book is about risk markers. Risk markers are measurable biochemicals, present in your blood, that are causally associated with atherosclerosis. These risk markers identify the biochemical or molecular causes of the disease. Because they provide information about the disruption of normal cellular processes that give rise to atherosclerosis, measuring risk markers provides a rational basis for treatment. If this treatment is instituted at an early stage in the disease process (for example, before symptoms appear), the disease is considered preventable. If treatment is instituted after symptoms appear, the disease is usually still reversible, but accomplishing this is slower and more difficult.
Risk factors should not be confused with risk markers. Risk factors are behaviors, dietary practices, symptoms, signs, diseases, or genetic predispositions that are associated with a statistically greater risk of atherosclerotic cardiovascular disease. These risk factors are based on population statistics, but are not necessarily causally related to the disease and therefore have no predictive value beyond statistical probability.
One way of viewing the difference between risk markers and risk factors is this: If you have a risk factor for heart disease, you might belong to the group with a higher statistical probability of developing the disease. On the other hand, if you have an abnormal risk marker, you know that the disease process (in this case, hardening of the arteries leading to stroke and heart attack) is developing in you.
This book is about the six most important risk markers for atherosclerotic disease. These tests identify the culprits that actually cause heart attacks and strokes. The following is a list of the known risk factors that are statistically - but not necessarily causally - associated with atherosclerotic disease:
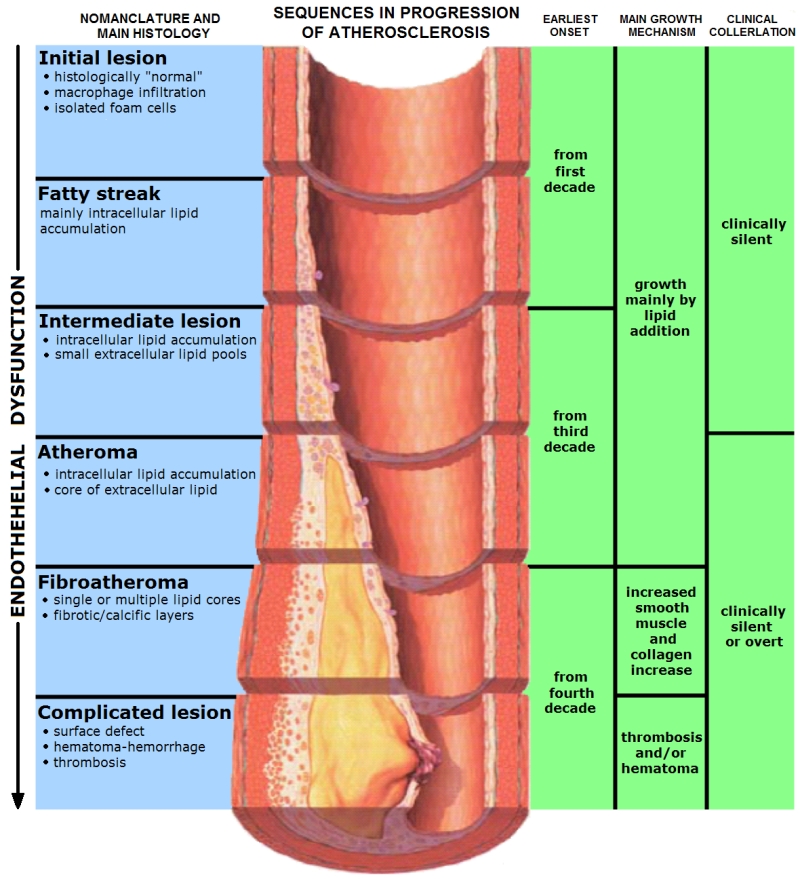
Atheromas develop gradually. The American Heart Association has identified six stages: